| |
| Volume 16, Number 2 | July 3, 2026 |
Until further notice, new bottles of Dr. Aardsma's Anti-Aging Vitamins dietary supplement shipped to customers from Aardsma Research & Publishing (ARP) will be formulated to provide an intake of 125 μg MePiA in the usual 8 daily drops of the supplement consumed by adult males.
Since this change renders previous bottles of Dr. Aardsma's Anti-Aging Vitamins dietary supplement unsatisfactory for further use, I have instructed our Marketing Department to exchange customers' old bottles, whether full or partially empty, for new bottles. The new bottles are necessarily more expensive than the old because MePiA is expensive to produce and it has now been increased by a factor of 125. Nonetheless, exchange of old for new will be free of charge.
The most important single piece of background for the present article is the reminder that:[1]
Unfortunately, determination of the optimal daily intake for vitamins in general is no trivial task. Scientists today are still working to fine tune the daily recommended intake of vitamins discovered several generations ago.The present article represents further progress in the ongoing effort to pin down the optimal daily intake of vitamin MePiA. I have been at this now for less than a decade, not several generations.
Beyond this are two foundational guidelines.
First, in the pre-Flood period, when humans were living to 925 years on average, the maximum daily intake had to have been less than 400 micrograms per day (μg/day).[2]
Second:[3]
[T]he optimal dose of MePA will likely be found to be within a factor of ten of a few micrograms per day.This quote mentions only MePA, but it applies equally to MePiA. The anti-aging vitamins were introduced to the modern world nine years ago via the first edition of Aging Cause and Cure.[4] At the time when the above quoted sentence was written, there was thought to be just one anti-aging vitamin, MePA. But, two years later, the discovery of a second anti-aging vitamin, MePiA, was announced.[5] The production of the two vitamins in the environment was nearly identical, making them a vitamin duo from the environmental perspective. (From a physiological perspective, from the very beginning they were recognized to be sharply distinct.)
The twin-like environmental behavior of the anti-aging vitamins allows them to be interchanged in some calculations. This is true of the environmentally-based calculations in Aging: Cause and Cure leading to the two foundational guidelines given above. These two guidelines may be summarized by saying that the final optimal daily intakes for both MePA and MePiA will certainly be less than 400 μg/day and (taking the quantitative limits of "a few" to mean 3–5) likely somewhere between 0.3 and 50 μg/day.
The recommended daily intake (RDI) of MePiA for adult males has ranged between 1 and 20 μg/day in the past, well within these guidelines. The present article raises MePiA's RDI to 125 μg/day. This increase results from a renewed commitment to a "confidently enough" policy,[6] spurred by recent progress in the understanding of MePiA's role in the body,[7] together with the experimental data presented below.
This new RDI for MePiA is a factor of 3.2 below the maximum guideline, but it is a factor of 2.5 above the upper end of the "likely" range guideline. This puts it outside this range for the first time, drawing attention to the fact that it is likely larger than the natural daily intake of MePiA by pre-Flood individuals. Emulating the pre-Flood intake has been an overarching principle for Dr. Aardsma's Anti-Aging Vitamins dietary supplement from the beginning because what pre-Flood individuals were doing was obviously working well, resulting in normal life spans of nearly a thousand years.
It is necessary to go to this larger-than-expected RDI because we moderns have suffered total dietary deprivation of MePiA all our lives and thus have some substantial catching up to do relative to pre-Flood individuals. We really need to be sure that our bodies are getting all the MePiA they can possibly use. To be certain that MePiA deficiency disease has been cured in our body—to be certain that we have rid ourselves of modern human aging entirely—we need to be certain that our body pool of this vitamin is completely replenished as rapidly as possible. This is essential to the cure of modern human aging.
The theory of the role played by vitamin MePiA in the body has come a long way, but it is still not complete.
Because MePiA is a phosphinate, and because phosphinates are known to play essentially zero role biologically,[8] it has been clear since very early on that the role of vitamin MePiA is not one of enabling biochemical reactions the way the traditional vitamins do. Because MePiA was known to be relatively easily oxidized, it was postulated instead to function exclusively as an antioxidant within the body.[9] Denham Harman's mitochondrial free radical theory of aging further narrowed its role to antioxidant activity within mitochondria.[10]
Modeling of biblical life span data revealed early on that MePiA had an extraordinarily long biological half-life.[11] This fact was utilized last issue to narrow MePiA's role to front-line defense against free hydroxyl radicals (OH·) in the mitochondrial matrix.[12] Remaining to be elucidated is exactly how MePiA fulfills this front-line defensive role. We know how MePiA is able to quench OH· to a harmless water molecule. The question to be answered next is how MePiA's ability to do this is actuated within the mitochondria.
Mitochondria have two membranes separating them from the rest of the cell. Inside the inner membrane, filling it up, is the matrix. The matrix is simply an aqueous solution of many different kinds of biomolecules. One important type of biomolecule in the matrix, for example, is mitochondrial DNA (mtDNA). It is one of a set of genetic biomolecules found there. These store and transmit the instructions for assembling many different types of proteins, which function as the central workhorses of the mitochondria. Also present in the matrix are antioxidants like vitamin C and glutathione. Then there are the energy carriers like NAD+ and ATP. All of these biomolecules and more play important, highly specific roles in the complex biochemical machine we call a mitochondrion.
Hydroxyl radical is deleterious—toxic—to mitochondria because it is very chemically reactive. This means that OH· is able to react with biomolecules. Reacting with a biomolecule changes it, making it no longer suited to its intended job. As a very simple analogy, automobiles are mechanical machines for transportation. Now imagine a mindless welder let loose on your automobile. He can weld metal pieces together on your automobile. You pull up to the gas pump to fill up the gas tank, but discover that you can no longer open the gas cap cover. It has been welded shut. This hinged cover can no longer do its specialized job. As a result, you can no longer fill the gas tank. As a result, the automobile runs out of gas, and is no longer able to do its transportation job. This is the impact of OH· on mitochondria. OH· must be stopped.
The simplest theory (Theory #1) for how MePiA acts to stop OH· in the matrix is via global interaction. Whenever and wherever OH· appears in the matrix, MePiA is there to deactivate and diffuse it.
For this theory to work, MePiA needs to be ubiquitous within the matrix. Hydroxyl radical is produced from hydrogen peroxide (HOOH), and HOOH is a small molecule which may diffuse anywhere and everywhere within the matrix. The matrix has significant apparatus designed to keep HOOH levels as low as possible, but this does not achieve zero HOOH, so HOOH can, in principle, show up anywhere in the matrix. This means that OH· can show up anywhere in the matrix. The extreme reactivity of OH· means that, once formed, it will react chemically more or less instantly with whatever biomolecule is near at hand. Thus, for Theory #1 to work, MePiA must be made so abundant within the matrix that hydroxyl radical is more likely to encounter and react with it than with any other molecule.
The large water solubility of MePiA (691 g MePiA/L H2O),[13] together with its small size (80 g/mole), make this strategy a real possibility. MePiA can furnish about five times more protective molecules per unit volume than vitamin C for example (330 g/L and 176 g/mole). But this strategy fails because the large quantity of MePiA needed appears impossible to furnish.
MePiA cannot be synthesized by the body. It is strictly an exogenous vitamin. And it has been clear from early on that the natural environment would have been able to furnish MePiA to the diet only in tiny amounts per day. As mentioned above, 400 μg MePiA per day is the maximum that can possibly have been furnished prior to the Flood. So a person living 925 years before the Flood would have taken a total of less than (400 * 365.25 * 925 =) 135 grams of MePiA by the time they died. This, as it turns out, is small compared to the amount of MePiA needed for it to be suitably ubiquitous in the matrix to protect against OH·.
Here is the calculation. I have used AI to look up the various numbers needed.
First, notice that it is impossible to deactivate 100% of OH·. To cut OH· damage to the mitochondria in half requires that the existing mass of non-water molecules in the matrix be matched by an equal mass of MePiA in the matrix. This would result in a 50% probability of OH· reacting with MePiA and 50% of reacting with non-MePiA molecules.[14] To really do the job of protecting against OH·, the mass of MePiA should probably be ten times that of the non-water molecules. To prevent all damage to the mitochondria would require the mass of MePiA to be infinitely larger than the non-water molecules.
To give a feel for the amount of MePiA which is needed, I will calculate the case of reducing OH· damage in half.
First, we need the total mass of mitochondria in the body. I was surprised to learn how large this is—10% of body weight. For a 70 kg adult, this yields 7 kg of mitochondria, including water.
Now the question becomes, what is the dry weight of mitochondria? Water is not a target of OH·. The dry weight has been measured. AI says 25–30% of total weight is dry weight. This gives (27.5 / 100 × 7 =) 1.9 kg.
This will still be somewhat too large because it includes the outer membrane, which is not a target of OH· in the matrix. So let us exclude items from the dry weight which are not targets.
AI gives a list of dry weights for liver cells (taken as typical of the body as a whole): matrix = 67%, inner membrane = 21%, outer membrane = 6%, intermembrane space = 6%. We want the whole matrix plus half (the inside) of the inner membrane, which is (67 + 21/2 =) 77.5% of dry weight. So the total weight of MePiA needed to match the hydroxyl-targeted dry weight is (1.9 × 77.5/100 =) 1.5 kg.
This is 1,500 grams, over ten times larger than the 135 g maximum that a male could ever have gotten over his entire 925-year life span before the Flood calculated above.
Theory #1 is, in this way, falsified. The body pool of MePiA needed to make Theory #1 work is much too large compared to the naturally available source rate.
The failure of Theory #1 teaches us that MePiA must somehow be localized to one or more regions in the matrix where it can do the most good. There are numerous possible versions of this theory at this stage. One can imagine, for example, arranging for a shield of MePiA molecules to be kept around mtDNA molecules to protect them from free hydroxyl radical damage in their vital role of information storage. Or one can imagine, as a second version, MePiA molecules operating as cofactors with enzymes which trap HOOH at its source, primarily near Complex I and Complex III of the electron transport chain, the enzymes deliberately reacting HOOH with a metal ion to yield OH· which is then immediately deactivated by the MePiA cofactor. Or one can imagine, as a third version, the neatly efficient, enzyme-assisted reaction of MePiA directly with HOOH yielding H2O plus MePA. From a strictly aesthetic perspective, this is my favorite version at present, though it faces the seemingly severe difficulty of how MePA gets recycled back to MePiA, as discussed last issue.[15]
The exact specifics of Theory #2 are not clear at present. This is the current frontier of the overall theory of the role played by MePiA in the body. But for the present purpose, knowledge of these specifics is not necessary.
All localized schemes, regardless of specifics, require that MePiA be somehow assisted. MePiA is not blindly diffusing about in the matrix in such schemes. Rather, something is keeping it where it is most needed.
Localizing MePiA shrinks the size of the body pool of MePiA needed to do the job. Take the hypothetical case of MePiA shielding the mtDNA, for example. Here, the mass of MePiA required to do the job would need to be at least as large as the whole-body mass of mtDNA itself. AI says that the weight of mtDNA is "estimated to be <1% (typically around 0.1% to 0.5%)" of the dry weight of the mitochondria. So the minimum mass of MePiA needed in the body in this case is (0.1/100 × 1.9 kg =) 1.9 g. This is 71 times smaller than the previously calculated 135 g maximum for pre-Flood males.
Theory #2 does not get falsified by the size of the body pool needed to do the job in its case, but the size of the body pool needed in the example mtDNA case just calculated is still surprisingly large. The largest MePiA RDI Dr. Aardsma's Anti-Aging Vitamins has had in the past is 20 μg per day. How long would it take to fill an initially empty body pool of 1.9 g at this rate of intake? The answer is (1.9/20×10-6 =) 95,000 days, which is 260 years! This result raises the possibility that the body pool of MePiA may not yet be filled for users of Dr. Aardsma's Anti-Aging vitamins.
Please notice that this is only a possibility, not a certainty. At present, the actual size of the body pool of MePiA is not known. The local interaction theory allows it potentially to be quite small.
But even the possibility that it is not small is still a game-changer. Before the progression of aging symptoms in mid- through late-life users of Dr. Aardsma's Anti-Aging Vitamins can be blamed on microheteroplasmy or CD38 overexpression or any other aging-induced disease,[16] the possibility must be eliminated that it is simply due to residual MePiA deficiency disease caused by a large MePiA body pool which has not yet been filled up. Successful treatment of CD38 overexpression disease requires that mitochondria first be fully replenished with MePiA. Substantial prior theory and discussion, together with the direction of research they instigated, must be tabled until this matter has been cleared up.
From very early on, the body pool of MePiA has been assumed to be small and easily filled. This assumption resulted first of all from the expectation that MePiA would have been much less abundant than MePA in the pre-Flood environment.[17]
Vitamin MePiA is an antioxidant. Because it is relatively easily oxidized to stable MePA, its concentration in natural sources of pre-Flood drinking water, such as lakes and rivers, is expected to have been much lower than the concentration of MePA. Thus it is expected that MePA will ultimately be found to have the larger RDI of the two vitamins.This expectation was augmented by an observation. My chronic inflammatory demyelinating polyneuropathy (CIDP) was cured in a matter of a few weeks by intake of 1 μg of MePA per day. This is a millionth of a gram of MePA per day, implying that the body pool of MePA must be quite small—way under a gram. And if the body pool of MePA appeared to be small and easily filled, the expectation was that the body pool of the less abundant MePiA would likely be even smaller.
This expectation was strengthened by my first measurements of excreted MePA, demonstrating that an intake of 20 μg MePA per day was more than enough.[18]
Known dietary sufficiency of MePA does not guarantee dietary sufficiency of MePiA. To guarantee dietary sufficiency of MePiA requires independent measurement of excreted MePiA, which has not yet been accomplished. However, the extraordinarily long biological half-life of MePiA (135 years)[19] suggests that the daily intake of this vitamin needed to meet physiological demands is likely to be extremely small, and this implies that the daily demand for MePA is likely to be larger than the daily demand of MePiA. Since Dr. Aardsma's Anti-Aging Vitamins dietary supplement supplies both vitamins in equal amounts, the present confirmation of its sufficiency with respect to MePA lends substantial weight to the expectation of its sufficiency with respect to MePiA as well.
The measurement of urinary excretion of MePiA was hindered by lack of a commercially available isotope standard for MePiA. Eventually, I made a quick spot-check measurement by first converting the MePiA in a urine sample to MePA. The difference in MePA before and after conversion of MePiA gave a quantitative measure of urinary excretion of MePiA.[20]
The concentration of MePiA excreted in human urine has now been successfully measured. This is the first such measurement that I am aware of. Most of the daily intake of MePiA was found to be present in the urine, confirming expectations once again.
The quantitative estimates of body pool size calculated above call all of this into question. A deliberate, thorough examination of whether the MePiA body pool has yet been replenished in any user of Dr. Aardsma's Anti-Aging Vitamins is clearly called for.
I launched an experiment involving a set of urinary excretion measurements to investigate this question in early March of this year. The idea was to test for dietary sufficiency in myself using a large trial intake of MePiA with subsequent measurements of excreted MePiA. If little of the trial dose was found to be excreted, this would be a clear indication that the body pool was not yet filled up.
As is usual in experimental research, development of a reliable measurement method was a protracted affair. Tandem mass spectrometry was used as the measurement method once again, as it had been for MePA four years ago.[21] To overcome the lack of a commercial isotope standard, needed for this measurement method, I was ultimately able to synthesize my own isotope standard (designated MePiA*).[22] The measurement was made as a negative ion parent scan of masses 79 Da and 80 Da for the positive ion daughter having a mass of 63 Da.[23] There was no interfering background ion in this instance as there had been with the MePA measurement, simplifying sample preparation. A 2 ml sample of the urine to be measured was used for each measurement. The complex urine sample matrix of the 2 ml, isotope-standard-labeled sample was removed prior to measurement via a strong anion exchange column.[24]
Method development was completed in late April. I had used myself as volunteer for the development process, six times taking 1,900 μg of MePiA, collecting total urine output day and night for several days after each dose, then measuring the amount of MePiA excreted in the urine. I experienced no adverse health events from these large doses. The quality of my measurement data was poor, however, especially early on as I developed the method. This complicated their interpretation.
To get an uncomplicated set of data on a typical user of Dr. Aardsma's Anti-Aging Vitamins, Helen (my wife) volunteered for the next round of measurements. The results are shown in Figure 1.
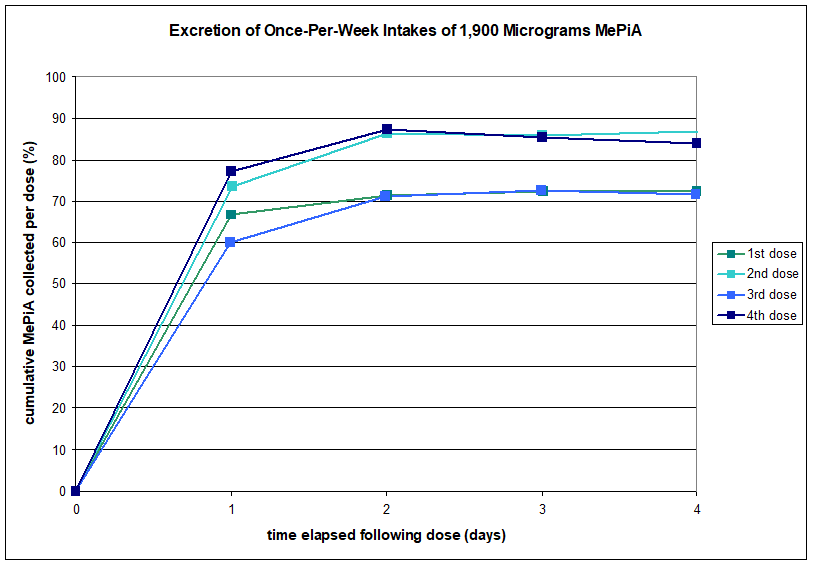 |
The main thing to notice with this graph is that most of the dose was excreted in all cases. Actually, more is excreted than is shown. These measurements track only urinary excretion. There will also be some fecal excretion. So total excretion was well above 70% in all cases. Thus, this set of measurements did not reveal a depleted body pool.
The scatter in the final total excretion results from one dose to the next is large. This is not yet explained. The first dose topped out at just 72%. When the second dose topped out at 87%, it seemed possible that some amount of replenishment might be going on, and that subsequent doses would top out at yet higher percentages as the body pool filled up. But then the third dose came in lower and very similar to the first dose, contrary to this idea. Adding to the confusion, the fourth dose behaved similar to the second dose. There seem yet to be uncontrolled experimental factors affecting the measured excretion percentages, such as the volume of water consumed each day by the volunteer, or the timing of consumption of solid foods following each dose. Further method development involving multiple volunteers would likely be needed to iron out all such factors. Nevertheless, the conclusion that this set of measurements did not reveal a depleted body pool seems robust.
There is one detail evident in Figure 1 which must be mentioned before moving on. Urinary excretion took two days to complete. This is true for all four doses. This seems significant.
According to AI, the kidneys are capable of completely eliminating a small, water-soluble acid within an hour or two of ingestion. AI says that a large dose of vitamin C—another small, water-soluble acid—may be expected to be eliminated within a half day of ingestion. Something is obviously holding back MePiA once it enters the body, keeping it from being rapidly eliminated by the kidneys. This seems to be an indication that the body "wants" MePiA. The body is not in a hurry to get rid of it.
I suggest that what is going on in this case is exactly what should be going on. After we ingest MePiA, it rapidly enters the bloodstream. If it stayed in the bloodstream, it would rapidly be eliminated from the body by the kidneys. Evidently, it does not stay in the bloodstream.
But, of course, it cannot stay in the bloodstream. According to the theory of modern human aging, MePiA is needed in the mitochondria and only in the mitochondria.[25] The mitochondria are located inside of cells. Thus, to get into the mitochondria, MePiA must enter the cells. It absolutely must move out of the bloodstream and into the cells.
The two-day elimination time for MePiA shows that the cells are receptive of MePiA. The cells need MePiA for their mitochondria. Thus, MePiA is free to enter the cells, traveling from the bloodstream through the cytosol of the cell to the mitochondria.
MePiA does not participate in any of the biochemistry going on in the cytosol, and so it produces no metabolites. It is a phosphinate, and thus it is inert to normal biochemical interactions. Its utility is all about antioxidant activity in the mitochondria, where its presence is essential to health and longevity.
It does not remain in the cell forever. It is free to leave the cell and reenter the bloodstream. If it is not taken up by the mitochondria, it will eventually get back into the bloodstream and be eliminated by the kidneys. But its excursion into welcoming cells significantly delays this outcome.
In this detail, these excretion data corroborate the theory of modern human aging.
Initially, I was surprised at the failure of Experiment #1 to reveal a depleted MePiA body pool. The calculations of the body pool size of MePiA discussed above had caused me to suspect that the body pool was, in fact, depleted. I had expected Experiment #1 to show this. It slowly dawned on me that transport of MePiA from the cytosol into the mitochondria was likely bottlenecked so that, while Experiment #1 had failed to reveal a depleted MePiA body pool, this did not constitute proof that the body pool was full. That MePiA transport is likely bottlenecked at the mitochondria may be seen as follows.
The cell is surrounded by a membrane. This membrane serves to keep cell stuff inside, and it serves to keep unwanted stuff outside.
Some substances easily cross the cell membrane. For example, O2 easily diffuses through the membrane from the blood into the cell, and CO2 easily diffuses from the cell back into the blood.
At the other end of the spectrum, charged substances (i.e., ions) face substantial resistance to crossing the cell membrane. For wanted ions, special transport mechanisms are built into the cell to get them across its membrane.
MePiA, at physiological pH, exists as nearly 100% negative ions. For it to cross the membrane, special transport mechanisms are essential.
We have just seen that such mechanisms must exist, because the Experiment #1 excretion data show that MePiA excretion is significantly delayed, implying significant time spent inside cells.
Mitochondria have a double membrane: an outer membrane and an inner membrane. While the difficulty of passage of small charged molecules through the outer membrane is similar to that of the cell membrane, the inner membrane is yet more difficult for them to cross. Specific transport proteins are required for them to cross the inner membrane, and this means that transport of MePiA into mitochondria is very likely to be bottlenecked at the inner membrane.
The design of the transport system for MePiA into the mitochondria would have been optimized for pre-Flood conditions. These conditions, we know, would likely have furnished the body with between 0.3 and 50 μg of MePiA per day. The implication is that the body will possess only sufficient MePiA transporters to bring this much MePiA into the total pool of mitochondria each day. Thus, the rate of transport of MePiA into the MePiA body pool is capped at probably less than 50 μg per day.
This means that a large, single dose of MePiA, like the 1,900 μg used in Figure 1, will mostly not be absorbed. The problem is that the body lacks the large number of transporters needed to move such a large dose from the cytosol into the mitochondria before most of it has been eliminated.
There is only one way to fill up the body pool of MePiA: daily supplementation at the limit the body can handle each day for however long it takes to fill it up.
This raises an exceedingly important question. How long is this likely to be?
Optimal design requires that this be fast enough to keep a developing human body, from zygote to adulthood, from suffering undue damage due to free hydroxyl radicals. AI says that the number of cells added per day is greatest from the third trimester of pregnancy through the first few months after birth. During this interval, body mass increases by as much as 0.07 kg/day. For a modern adult male weighing 70 kg, this implies that replenishment of MePiA starting from zero MePiA will take (70 / 0.07 =) 1,000 days, which is 2.7 years.
This calculation is an approximation only. It uses total body mass where what is really of interest is total mitochondrial mass. AI reveals that there is a large spike in the growth of mitochondrial mass immediately following birth as the cells switch over from glycolysis to oxidative phosphorylation with the advent of more abundant oxygen supply to tissues due to the onset of breathing. So mitochondrial mass is not always the same proportion of total body mass all through life the way the calculation assumes. The calculated 2.7 years should be treated as a ballpark figure only, not as a precisely known time for replenishment. It indicates that replenishment for modern mature adults, who have grown up all their lives with zero dietary MePiA, will likely take more than a year and less than a decade when supplemented optimally.
At the opposite end of the age scale, the above calculation incidentally implies that there is a large need for dietary MePiA with the newborn. Optimal design suggests that this demand would naturally have been met pre-Flood by MePiA ingested by the mother and furnished to the baby in optimal amounts via her breast milk. For this reason, mothers are advised not only to take Dr. Aardsma's Anti-Aging Vitamins but also to breastfeed their infants and toddlers. No studies of MePiA concentrations in breast milk have yet been performed. This makes it impossible to make any informed recommendation at present regarding MePiA in infant formula, for example. The safest practice at present is simply to breastfeed, as would have been the case pre-Flood.
Beyond this is the additional recommendation that sugar water not be administered to the newborn.[26] The mother (like everyone else) should be taking daily MePiA via Dr. Aardsma's Anti-Aging Vitamins, and no competitor with her breast milk should be introduced to the infant, most especially in the interval of heightened mitochondrial biogenesis immediately following birth.
Having found that most of a large dose of MePiA would be excreted, the next question became just how much MePiA the body could absorb per day. Synthesis of MePiA having a purity suitable for human consumption is expensive. There is no point in taking MePiA just to have it excreted. Meanwhile, it is clearly important to be confident that the body is getting all the MePiA it can use each day. What is the daily intake which confidently meets daily need while minimizing waste and expense?
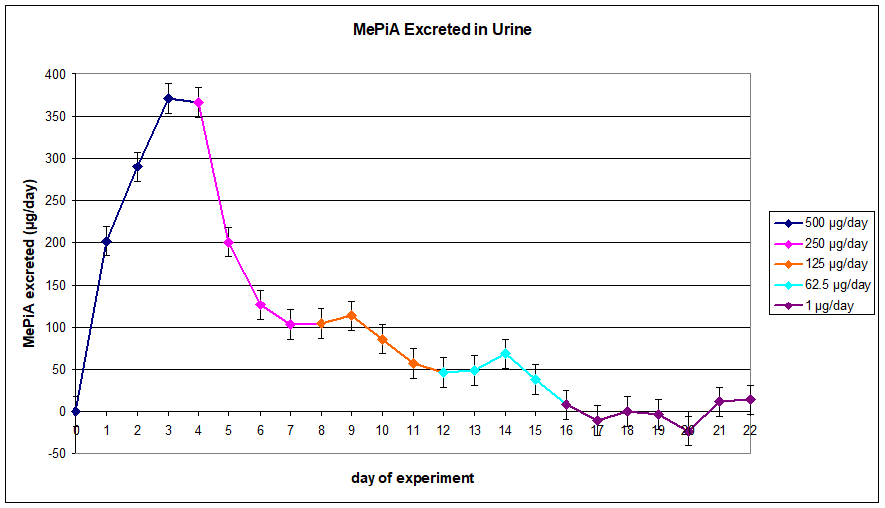
To answer this question I launched a second set of measurements on myself to monitor excreted MePiA at periodically diminishing doses. Figure 2 shows the results.
 |
Before I answer the main question using these data, there are two preliminary observations which need to be discussed.
First, notice that these data show that it takes three days for a large dose to be eliminated in my case, compared to the two days required in Helen's case discussed previously. This difference seems certain to be a result of greater hydration in Helen's case than in mine. Helen drinks much more water per day than I do. The result is more urine per day in her case, which means that she rinses out her bloodstream more rapidly than I do.[27]
Second, I changed my mode of taking my daily MePiA intake starting with the 250 μg/day intake on Day 4. For the 500 μg/day dataset, I took the daily dose in half a cup of water 45 minutes before breakfast. For the remaining data points, I took the daily dose with breakfast.[28] This change made a large difference to urinary versus fecal excretion. When taken 45 minutes before breakfast, 74% was excreted in the urine. When taken with breakfast, only 42% was excreted in the urine. The difference, 32%, would be due to additional fecal excretion when taking the dose together with food.
Back to the main question. The major outcome was the finding that the new RDI for MePiA should be 125 μg per day. This was determined as follows.
First, with the total final dataset in hand, I used the data points from the last four days of the experiment (Days 19–22) to determine the measurement uncertainty. The standard deviation of these four data points was calculated to be 17.4. This calculated, one-standard-deviation (1σ) uncertainty was then added to the graph as error bars on all of the data points.
Then I found the smallest of the tested daily intake regimens which could be depended on, at greater than 95% confidence level, to provide more than enough daily MePiA as evidenced by non-zero daily urinary excretion. Working from smaller to larger, I found that 1 μg/day clearly did not achieve statistically significant excretion different from 0 μg. The error bars on the graph for the 1 μg/day regimen illustrate this, most overlapping the zero μg/day, X-axis line. The next higher intake, 62.5 μg/day, gave 8 ± 17.4 μg/day after four days, which is obviously not different from zero at 95% confidence level. The error bar on the day 16 data point shows this, once again overlapping the X axis.
The next higher intake, 125 μg/day, gave 47 ± 17.4 μg/day after four days, which is statistically different from 0 at 99% confidence level. This says that 125 ug MePiA/day may confidently be depended on to provide more than enough intake of MePiA based on these urinary-excretion data.
This gives the new RDI for MePiA of 125 μg/day.
I know of no health safety concern, either experimental or theoretical, at this new RDI. Though the increase is large relative to the previous RDI, the actual amount of MePiA being taken each day is still tiny—125 millionths of a gram.
Safety data for MePiA have previously been reviewed for the New Dietary Ingredient Notification submitted to the FDA for Dr. Aardsma's Anti-Aging Vitamins dietary supplement.[29] These data showed MePiA to be a dietarily safe substance, even in amounts thousands of times larger than are used in Dr. Aardsma's Anti-Aging Vitamins.
The acute oral toxicity of MePiA was formally evaluated via standard LD50 tests in laboratory rats. The results showed an LD50 of 940 mg/kg body weight (BW) with a 95% confidence interval of 476 to 1858 mg/kg BW [body weight]. This places the acute oral toxicity of MePiA 1.9 times lower than the 501 mg/kg BW minimum required for a compound to be considered to be in the low acute oral toxicity category. For general reference on the toxicity scale, comparing to other oral LD50 values in rats, the LD50 of MePiA is 3.2 times more toxic than table salt (NaCl), and 4.9 times less toxic than caffeine.
In addition to being of low acute oral toxicity, MePiA is not mutagenic.
MePiA does not display chronic toxicity. MePiA will be highly dissociated at physiological pH based on its pKa value (pKa = 3.08), and will therefore not bioaccumulate over time. Experiments with mice (designed to look for increased longevity rather than toxicity) reveal only increased longevity and no evidence of chronic oral toxicity. For example, supplementation of the diets of 27 Hsd:ICR female mice at 100 mg MePiA/liter drinking water beginning at 24.7 weeks of age and ending at 109.6 weeks of age increased maximal life span by 20% relative to the control group not treated with MePiA. This is equivalent to a human intake of roughly 250,000 μg MePiA per day.
Previous concerns about a possible upper limit for MePiA appear to be unfounded.[30] These concerns were based on a theoretical possibility of MePiA interference with ROS signaling.
This theoretical consideration disappears once it has been understood that the antioxidant role of MePiA is restricted to quenching OH·, as is now the case.[31] While OH· is a member of the ROS family, it does not possess a signaling role the way superoxide and hydrogen peroxide do. Interference with ROS signaling systems outside the mitochondria is thus not a concern in its case.MePiA appears at present to function exclusively as an antioxidant, and its antioxidant activity appears to be utilized exclusively within mitochondria where it is essential to their maintenance, its job being to neutralize reactive oxygen species (ROS) produced as unwanted side-products of normal respiration.
But the role played by ROS in the body in general is not exclusively bad. ROS are used outside the mitochondria as cellular signaling molecules, for example. This implies that physiologically excessive MePiA external to the mitochondria has potential to interfere with ROS signaling systems outside the mitochondria.
Said simply, there is no reason, either experimental or theoretical, for concern about the safety of MePiA consumption at the new RDI.
Helen and I have now both tested MePiA at the doses shown on the two graphs this issue. This includes six 1,900 μg doses for me over a three week period and four 1,900 μg doses for Helen over a four week period. It includes, for me, the 500, 250, 125, and 62.5 μg MePiA per day doses of Figure 2, each for four days running. We have also tested both 100 and 125 μg MePiA per day for over a month. Not surprisingly, we have experienced no adverse health events from any of this.
In fact, our experience has been the opposite. For the past several weeks, we both have been feeling that we are doing better. I am noticing tolerance of many foods which my IBS previously forbade. We are both noticing higher energy levels. We feel like we have turned a corner of some sort—that our health and strength are presently trending upward after a long spell of slow decline. This was not present with previous high-intake tests just a few months back, so it does not seem to be a result simply of a higher intake of MePiA—of more MePiA circulating in our blood. Rather, it seems possible that we have crossed a total cumulative absorbed intake threshold after months of high intake. A viable theory is that we are beginning to feel the impact of mitochondria which are starting to become more productive once again.
We now know that full MePiA body pool replenishment is likely to take years. But we feel very encouraged by this recent upturn. It is much more encouraging to look forward to years of improvement than years of ongoing decline. We hope this trend continues.
A renewed commitment to a "confidently enough" policy coupled to current theoretical understanding and experimental results produces a new RDI for MePiA of 125 μg MePiA per day.
It seems likely that this new RDI will be revised downward in the future as measurement precision improves at the very low levels needed to track urinary excretion when daily intake of MePiA is less than 100 micrograms. For the present, however, the priority is ensuring sufficient daily MePiA intake to replenish body stores as rapidly as possible. This is necessary to ensure a maximal rate of recovery from the MePiA deficiency disease component of aging. ◇
ZZZ1mbox
The Biblical Chronologist is written and edited by Gerald E. Aardsma, a Ph.D. scientist (nuclear physics) with special background in radioisotopic dating methods such as radiocarbon. The Biblical Chronologist has a fourfold purpose:
The Biblical Chronologist (ISSN 1081-762X) is published by: Aardsma Research & Publishing Copyright © 2026 by Aardsma Research & Publishing. |
^ Matthew P. Aardsma, "Intake Recommendations for Dr. Aardsma's Anti-Aging Vitamins," The Biblical Chronologist 10.10 (June 10, 2020): 2. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, Aging: Cause and Cure (Loda, IL: Aardsma Research and Publishing, 2017), 109. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, Aging: Cause and Cure (Loda, IL: Aardsma Research and Publishing, 2017), 111–112. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, Aging: Cause and Cure (Loda, IL: Aardsma Research and Publishing, 2017). www.BiblicalChronologist.org.
^ Gerald E. Aardsma, Addendum to Aging: Cause and Cure (Loda, IL: Aardsma Research and Publishing, July 26, 2019). www.BiblicalChronologist.org.
^ Matthew P. Aardsma, "Intake Recommendations for Dr. Aardsma's Anti-Aging Vitamins," The Biblical Chronologist 10.10 (June 10, 2020): 7. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "Vitamin MePiA's Role," The Biblical Chronologist 16.1 (June 9, 2026): 1–6. www.BiblicalChronologist.org.
^ William W. Metcalf and Wilfred A. van der Donk, "Biosynthesis of Phosphonic and Phosphinic Acid Natural Products," Annual Review of Biochemistry 78 (2009): 65–94.
^ Gerald E. Aardsma, Addendum to Aging: Cause and Cure (Loda, IL: Aardsma Research and Publishing, July 26, 2019), 11. www.BiblicalChronologist.org.
^ Denham Harman, "The Biologic Clock: the Mitochondria?" Journal of the American Geriatrics Society 20 (1972): 145–147.
^ Gerald E. Aardsma, Addendum to Aging: Cause and Cure (Loda, IL: Aardsma Research and Publishing, July 26, 2019), 12. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "Vitamin MePiA's Role," The Biblical Chronologist 16.1 (June 9, 2026): 1–6. www.BiblicalChronologist.org.
^ Obtained from go.drugbank.com via AI.
^ This calculation should really use volumes of molecules, not mass, but intrinsic densities of individual molecules are roughly the same, so mass is adequate for the present purpose.
^ Gerald E. Aardsma, "Vitamin MePiA's Role," The Biblical Chronologist 16.1 (June 9, 2026): 1–6. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "The End of Modern Human Aging Appears Imminent," The Biblical Chronologist 15.5 (November 11, 2025): 1–4. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "The RDIs for Vitamins MePA and MePiA Have Now Been Reduced," The Biblical Chronologist 12.2 (June 21, 2022): 1–2. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "First Measurement of Vitamin MePA Excreted in Human Urine Confirms Adequacy of RDI," The Biblical Chronologist 12.1 (April 26, 2022): 1–4. www.BiblicalChronologist.org.
^ Gerald E. Aardsma and Matthew P. Aardsma, Aging: Cause and Cure, 2nd ed. (Loda, IL: Aardsma Research and Publishing, 2021), 110. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "The RDIs for Vitamins MePA and MePiA Have Now Been Reduced," The Biblical Chronologist 12.2 (June 21, 2022): 1–2. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "First Measurement of Vitamin MePA Excreted in Human Urine Confirms Adequacy of RDI," The Biblical Chronologist 12.1 (April 26, 2022): 1–4. www.BiblicalChronologist.org.
^ Hydrolysis of diethyl methylphosphonite in pure D2O gave D-P in place of the usual H-P of MePiA. This raised the negative ion mass of MePiA from the usual 79 daltons (Da) to 80 Da for this isotope standard.
^ A mass 79 machine memory background, which changed sample by sample, was corrected for by measuring a zero sample (containing MePiA* only) immediately before and after each sample measurement.
^ Bio-Rad.com, Poly-Prep Columns, AG 1-X8, formate form #7316221.
^ Gerald E. Aardsma, "The End of Modern Human Aging Appears Imminent," The Biblical Chronologist 15.5 (November 11, 2025): 1–4. www.BiblicalChronologist.org.
^ This was standard practice in hospitals before the Baby-Friendly Hospital Initiative by the World Health Organization and UNICEF launched in 1991.
^ I don't spend much time thinking about hydration, but I am aware that hydration fads are currently prevalent. If pinned down on the topic, I would say that I expect that God equipped us with thirst sensors so that our bodies could regulate water intake according to what is best for each one individually. This is not meant to ignore the need to give deliberate thought and care to hydration in special situations such as sustained diarrhea or vomiting.
^ This mode is not only more convenient, it also more closely emulates what pre-Flood people would have done.
^ Gerald E. Aardsma and Matthew P. Aardsma, "The FDA New Dietary Ingredient Notification for Vitamin MePiA," The Biblical Chronologist 10.12 (June 23, 2020): 1–8. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "The RDI for Vitamin MePiA Has Now Been Reduced," The Biblical Chronologist 14.6 (April 3, 2024): 1–3. www.BiblicalChronologist.org.
^ Gerald E. Aardsma, "Vitamin MePiA's Role," The Biblical Chronologist 16.1 (June 9, 2026): 1–6. www.BiblicalChronologist.org.